Table of Contents >> Show >> Hide
- Complete Heart Block at a Glance
- What Is Complete Heart Block (Third-Degree AV Block)?
- Symptoms of Complete Heart Block
- What Causes Complete Heart Block?
- How Doctors Diagnose Complete Heart Block
- Treatment: From Urgent Stabilization to Long-Term Fixes
- Living With Complete Heart Block (and a Pacemaker)
- Outlook and Prognosis
- Prevention and When to Seek Care
- FAQ: Quick Answers People Actually Want
- Real-Life Experiences With Complete Heart Block (What People Commonly Report)
- Conclusion
If your heart had a customer-service department, complete heart block would be the moment the phone line between “upper management” (the atria)
and “the people who actually ship the product” (the ventricles) gets cut. The work still happensbut now everyone’s improvising, schedules don’t match,
and the whole operation can slow to a crawl.
Complete heart block (also called third-degree atrioventricular (AV) block) is a serious heart rhythm problem in which the electrical
signals from the atria don’t reliably reach the ventricles. Because the ventricles aren’t getting the usual “beat now” message, they often fall back on
a slower backup rhythm. That can reduce blood flow to the brain and the rest of the bodyleading to dizziness, fainting, shortness of breath, or worse.
The good news: modern treatment (especially pacemakers) can be very effective, and many people get back to living full, active lives.
Complete Heart Block at a Glance
- What it is: Total electrical disconnect between atria and ventricles (AV dissociation).
- How it feels: Often like “my battery is at 1%” fatigue, lightheadedness, near-fainting, or sudden blackout.
- Why it matters: The heart may beat too slowly to deliver enough oxygen-rich blood.
- Typical treatment: Temporary stabilization in urgent cases, then usually a permanent pacemaker.
- Outlook: Strongly depends on the cause, but outcomes often improve dramatically after pacing and treating the underlying trigger.
What Is Complete Heart Block (Third-Degree AV Block)?
Your heart runs on electricity. Normally, an impulse starts in the sinoatrial (SA) node (the “natural pacemaker”) in the atria, travels through the AV node,
and then moves down specialized wiring (the His-Purkinje system) to trigger the ventricles to contract. That sequence keeps the heart pumping efficiently.
In complete heart block, signals from the atria don’t make it to the ventricles. The atria continue to follow the SA node’s rhythm,
while the ventricles rely on a backup “escape rhythm” that tends to be slower and less dependable. When the ventricular rate drops too low, blood pressure
can fall and symptoms show upsometimes abruptly.
A quick mental picture: imagine two drummers in the same band who can’t hear each other. They both keep playing… just not together. That loss of coordination
can make the music (your circulation) sound like chaosor at least a very sleepy jazz set at 2 a.m.
Symptoms of Complete Heart Block
Symptoms vary. Some people notice subtle, creeping fatigue. Others get a dramatic “lights out” moment (syncope) because the brain is briefly under-supplied
with blood.
Common symptoms
- Lightheadedness or dizziness
- Fainting or near-fainting (syncope/presyncope)
- Fatigue and exercise intolerance (“I used to do stairs; now I negotiate with them.”)
- Shortness of breath, especially with activity
- Chest discomfort or pressure (especially if an acute heart problem is involved)
- Palpitations (awareness of an irregular or slow heartbeat)
- Confusion or “brain fog,” especially in older adults
- Low blood pressure, weakness, or feeling unusually cold/clammy
Red-flag symptoms: get urgent care
Because complete heart block can be an emergency, seek immediate medical help if you have fainting, severe shortness of breath, chest pain,
new confusion, or severe weaknessespecially if symptoms are sudden or worsening.
What Causes Complete Heart Block?
Complete heart block is a final common pathway: many different problems can interrupt the electrical connection between atria and ventricles.
Clinicians group causes into “structural,” “ischemic,” “medication-related,” “inflammatory/infectious,” “metabolic,” and “post-procedure.”
Finding the cause matters because some triggers are reversible.
1) Age-related conduction system degeneration (wear-and-tear)
Over time, the heart’s electrical “wiring” can develop fibrosis (scarring) that slows or blocks conduction. This is one reason heart block becomes more
common later in life.
2) Heart attack and ischemia
An acute myocardial infarction (heart attack) can damage the conduction system, causing new AV block. The pattern and persistence can vary by which artery
is involved and where the block sits (AV node vs. below it). Because this can be life-threatening, it’s treated as urgent.
3) Structural heart disease
Conditions that change heart structurecardiomyopathy, significant valve disease, or infiltrative diseasescan affect conduction. Sometimes the block is a
clue that there’s a bigger underlying heart condition worth investigating.
4) Medications and drug effects
Certain drugs can slow conduction through the AV node and may trigger or worsen heart blockespecially when doses are high, kidney function changes,
drug interactions occur, or the conduction system is already vulnerable. Common culprits include beta blockers, certain calcium channel blockers,
and digoxin (among others).
5) Post-surgery or post-procedure heart block
Heart surgery and some catheter-based procedures can temporarily or permanently affect conduction. This includes valve surgery and transcatheter aortic valve
replacement (TAVR), where the device sits near the heart’s conduction pathways. Not everyone develops complete heart block, but it’s a known risk in certain
settings.
6) Inflammatory and infectious causes
Myocarditis (inflammation of the heart muscle) and systemic/infiltrative diseases (like sarcoidosis or amyloidosis) can impair conduction.
Lyme carditis is a particularly important infectious cause in the U.S.: it can produce high-degree or complete AV block that may change
rapidly and is often treatable with antibiotics, sometimes with temporary pacing support.
7) Metabolic and other reversible triggers
Electrolyte abnormalities (like severe high potassium) and endocrine problems (such as significant thyroid dysfunction) can contribute to bradycardia or
conduction issues. Identifying these matters because correcting them may improve conduction.
How Doctors Diagnose Complete Heart Block
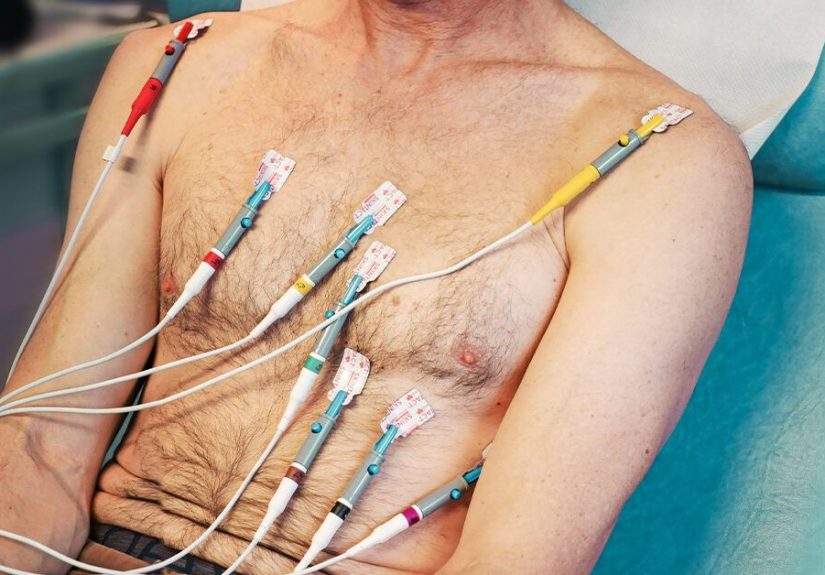
Diagnosis starts with history and vital signs (heart rate, blood pressure, oxygen levels), but the key test is the electrocardiogram (ECG/EKG).
Complete heart block typically shows AV dissociation: P waves marching through at their own rate, QRS complexes marching through at a slower
rate, and no consistent relationship between them.
Tests you might encounter
- 12-lead ECG: the snapshot that often makes the diagnosis.
- Continuous monitoring (telemetry): especially if symptoms come and go.
- Holter or event monitor: helpful when episodes are intermittent.
- Blood tests: electrolytes, thyroid studies, medication levels when relevant, markers of infection or heart injury when suspected.
- Echocardiogram (ultrasound of the heart): often used to assess structure and function when high-grade or third-degree AV block is newly identified.
- Additional imaging or electrophysiology evaluation: sometimes used when the cause is unclear or an infiltrative process is suspected.
A helpful “why” behind the testing: complete heart block isn’t just a rhythm label; it’s a symptom of somethingage-related fibrosis, ischemia, medication
effect, infection, or structural disease. The workup is designed to identify what can be fixed and what needs long-term pacing support.
Treatment: From Urgent Stabilization to Long-Term Fixes
Treatment depends on how stable you are, what your heart rate looks like, and what’s causing the block. Some people need immediate stabilization.
Others are stable enough for monitored evaluation and a planned pacemaker procedure.
Emergency and hospital management
If complete heart block causes dangerously slow heart rates, low blood pressure, chest pain, confusion, or fainting, clinicians treat it as urgent.
In the short term, the goal is to maintain blood flow to the brain and organs while determining the cause and arranging definitive treatment.
- Monitoring and IV access: continuous rhythm and blood pressure monitoring.
- Medications to support heart rate/blood pressure: drugs like dopamine or epinephrine may be used as temporary support in symptomatic bradycardia,
though they’re often a bridge rather than a cure. - Pacing support: transcutaneous pacing (pads on the skin) can be used quickly, and transvenous pacing (a wire through a vein) may be considered
in selected cases. Temporary pacing is generally kept as short as possible because it has meaningful risks. - Treat the trigger: stop or adjust medications that may be contributing; treat infection; correct electrolytes; manage acute coronary syndromes promptly.
A nuance that surprises people: atropine (a common first-line drug for symptomatic bradycardia) often doesn’t work well in complete heart block because it acts
mainly at the AV node, and the block may be below that level. Clinicians may still try it depending on the situation, but they don’t bet the whole plan on it.
The definitive treatment for most: a permanent pacemaker
For many patients, especially when the block is persistent, the most reliable long-term treatment is a permanent pacemaker.
A pacemaker is a small device placed under the skin (often in the upper chest) with leads that deliver electrical impulses to help keep the heart beating in a
safer rhythm.
Think of a pacemaker as a calm, consistent metronomeone that steps in when the heart’s natural timing system can’t keep the ventricles moving reliably.
The device can sense when the heart rate is too slow and send impulses to prompt a beat.
Addressing reversible causes (because sometimes the block isn’t forever)
Even when a pacemaker is needed, clinicians still hunt for reversible contributors. A few examples:
- Medication-related block: dose changes or stopping the offending drug can improve conduction in some cases.
- Acute MI-related block: restoring blood flow quickly may improve conduction, depending on the infarct pattern.
- Lyme carditis: appropriate antibiotics and monitoring can lead to recovery, and some patients only need temporary pacing support during treatment.
- Electrolyte or endocrine issues: correcting the imbalance can improve rhythm stability.
Living With Complete Heart Block (and a Pacemaker)
Once a pacemaker is in place and tuned correctly, many people notice a dramatic difference: less dizziness, better stamina, fewer “why am I so tired?” days.
Still, it’s normal to have practical questions about daily life, workouts, travel, and gadgets.
What recovery is often like
- Short-term soreness: the incision area can be tender for days to weeks.
- Arm movement limits at first: you may be asked to avoid certain overhead motions briefly to protect healing and lead position.
- Follow-up and programming: the device is checked and adjusted to match your needs (resting rate, exertion response, etc.).
Common lifestyle considerations
- Medical follow-up: regular checks (often including remote monitoring) help ensure the device and leads are working well.
- Magnets and devices: most everyday electronics are fine, but you’ll receive guidance about strong magnets and specific equipment.
- Travel and airport security: many people travel routinely; carrying your pacemaker card and following instructions for screening helps.
- Future maintenance: batteries don’t last forever; replacements are planned, not a surprise party.
The bigger message: a pacemaker doesn’t “make you fragile.” It’s more like a supportive teammate that keeps the rhythm steady so your body can do the things
you actually care aboutwalking the dog, dancing at weddings, or simply getting through a grocery run without needing a nap in aisle five.
Outlook and Prognosis
The outlook for complete heart block depends heavily on the underlying cause and how quickly it’s treated. Untreated third-degree heart block can be dangerous
because a very slow, unreliable rhythm can reduce blood flow and raise the risk of falls, injury, and in severe cases, cardiac arrest.
With appropriate treatmentoften pacing plus treatment of the underlying triggermany people do well. Those whose complete heart block is caused by a reversible
problem (such as certain medication effects or Lyme carditis) may recover conduction over time, though careful monitoring is essential.
Potential complications to know about
- Injury from syncope: falls and accidents are a major real-world risk before treatment.
- Heart failure symptoms: can occur depending on underlying heart disease and pacing needs.
- Pacemaker-related issues: infection, lead problems, or battery depletion (managed with follow-up and planned replacements).
Prevention and When to Seek Care
You can’t prevent every cause of complete heart block, but you can reduce risk by managing cardiovascular health and catching problems early.
Practical prevention moves
- Manage heart disease risk factors (blood pressure, diabetes, cholesterol, smoking).
- Review medications regularlyespecially if you develop new dizziness, fatigue, or a slow pulse.
- Seek care for symptoms after tick exposure, especially if you develop palpitations, fainting, or shortness of breath (Lyme carditis can progress quickly).
- Follow up promptly after cardiac procedures if you notice new lightheadedness, low heart rate, or fainting.
When to call 911 or get emergency care
Call emergency services for fainting, chest pain, severe shortness of breath, severe weakness, confusion, or a very slow heart rate with symptoms.
Complete heart block can be an emergency, and rapid evaluation matters.
FAQ: Quick Answers People Actually Want
Is complete heart block the same as a “blocked artery”?
No. “Heart block” refers to electrical signal conduction, not clogged arteries. A heart attack can cause heart block, but the term itself is about
electrical timing, not plumbing.
Can complete heart block come and go?
Yes. Some causes (medication effects, infections like Lyme, or post-procedure inflammation) can create block that fluctuates. That’s why monitoring is often
importanteven if symptoms seem intermittent.
Will I always need a pacemaker?
Many people with persistent complete heart block need a permanent pacemaker. However, in certain reversible situations (for example, Lyme carditis treated with
antibiotics), conduction can improve over weeks. Your cardiology team decides based on cause, stability, and how reliable your intrinsic rhythm is.
Real-Life Experiences With Complete Heart Block (What People Commonly Report)
Medical descriptions are neat and tidy. Real life is not. Here are experiences patients and clinicians often describe around complete heart blockwhat it
can feel like, what the hospital process is like, and what living with treatment tends to look like. (These are common themes, not a substitute for
personalized medical care.)
1) “I didn’t feel sickI felt… unplugged.”
A lot of people don’t start with dramatic chest pain. They start with a weird, creeping mismatch between effort and energy: walking across a room feels like
walking across a continent; showering requires a recovery plan. Some describe a heavy-headed sensationlike standing up too fast, but all day. Others notice
their pulse is surprisingly slow, or they feel momentary “blank spots” where their brain seems to buffer, like a streaming video on bad Wi-Fi.
2) The fainting can be sudden and rude.
Syncope from complete heart block can be abrupt: one moment you’re talking, the next you’re on the floor wondering why the ceiling looks so judgmental.
People sometimes mistake these episodes for dehydration, low blood sugar, or even seizuresespecially if there are brief twitchy movements during a faint.
This overlap is one reason clinicians take a detailed history and often check an ECG early.
3) The ER moment: “You’re not just tiredyour rhythm is slow.”
Many patients report relief when someone finally measures what they’ve been feeling: a very slow ventricular rate, low blood pressure, or a classic ECG
pattern. It can be scary to hear “complete heart block,” but it can also be clarifyingbecause now there’s a concrete reason for the symptoms and a
well-established path to stabilize things.
4) Temporary pacing is weirdly medievaland also lifesaving.
If urgent pacing is needed, patients often remember the pads (transcutaneous pacing) as uncomfortable but fast. It’s a bridge, not the destination.
Others receive temporary internal pacing in selected circumstances. People commonly describe the early phase as “a lot of monitors, a lot of beeping,
a lot of staff taking it very seriously,” whichwhen your ventricles are freelancing at 30–40 beats per minuteis exactly the correct vibe.
5) Pacemaker day: anxiety before, surprise afterward.
Pacemaker implantation can sound intimidating, but many patients are surprised by how quickly symptoms improve afterward. A common story is:
“I didn’t realize how bad I’d been feeling until I felt normal again.” Energy returns. The constant dizziness fades. Stairs become stairs again instead of
a personal betrayal. There can be soreness at the site and short-term movement restrictions, but the overall improvement in day-to-day function is often
the headline.
6) The mental shift: learning to trust your body again.
After episodes of fainting or near-fainting, people can become understandably cautiousavoiding driving, exercise, or being alone. Once the rhythm is stabilized
and the cause is addressed, rebuilding confidence is part of recovery. Patients often say that follow-up visits and device checks help them feel safe because
someone is “watching the watchman.”
7) When the cause is reversible, patience is part of the treatment.
People with causes like Lyme carditis often describe a different journey: hospitalization for monitoring, antibiotics, sometimes temporary pacing, and then a
gradual return of normal conduction over weeks. The experience can feel like a rollercoaster because the degree of block can change rapidly. The upside is
that recovery can be excellent when treated promptly.
The big takeaway from real-world experience is simple: complete heart block is serious, but it’s also one of those conditions where modern cardiology has a
strong toolkit. Getting evaluated quickly, finding the cause, and using pacing when needed can turn a frightening diagnosis into a manageable chapter.
Conclusion
Complete heart block (third-degree AV block) happens when the heart’s electrical signals can’t travel from atria to ventriclesforcing the ventricles to rely
on a slower backup rhythm. Symptoms often include dizziness, fatigue, shortness of breath, and fainting, and it can be an emergency. Causes range from age-related
conduction system fibrosis and heart attacks to medication effects, post-procedure conduction injury, and infections like Lyme carditis. Diagnosis centers on ECG,
and treatment typically involves urgent stabilization when needed and, in persistent cases, a permanent pacemakerplus targeted therapy for reversible triggers.
With timely care, many people regain stability and quality of life.